MedConsult AI: The Clinical Intelligence Layer
How AI-assisted consultation, secure documentation, and compliance-grade controls eliminate the documentation burden without compromising the physician-patient relationship.
“The documentation burden in modern healthcare is not a data problem. It is a cognitive tax on the people best positioned to prevent it — and the only sustainable solution is intelligence that understands clinical context, not just clinical data.”
Paper DNA
Domain
Healthcare AI
Maturity
Live
Market Size
Clinical documentation $5.7B · US healthcare $4.3T
Connected To
MedConsult AI targets the $5.7B clinical documentation software market with an AI-native architecture that replaces clipboard-style EHR data entry with intelligent ambient documentation — capturing, structuring, and securing clinical encounters in real-time.
The compliance moat is structural: HIPAA-grade encryption, PHI data isolation per tenant, and an immutable audit trail that makes MedConsult AI the only AI consultation tool a regulated healthcare enterprise can deploy without a legal review cycle.
The go-to-market wedge is documentation burden relief — the most universally felt pain across all care settings — creating a land-and-expand dynamic from individual practitioners to group practices to enterprise health systems.
The Documentation Crisis in Modern Healthcare
American physicians spend 1.84 hours on administrative documentation for every hour of direct patient care. Emergency medicine physicians document for 43% of their shift. Primary care physicians open their EHR an average of 45 times per day and spend 6 hours of an 11-hour workday on the keyboard. This is not a productivity problem. It is a structural misallocation of the most expensive and irreplaceable resource in the healthcare system.
The consequences are not abstract:
| Consequence | Scale |
|---|---|
| Physician burnout | 63% of US physicians report symptoms — documentation cited as primary driver |
| Diagnostic time lost | Each EHR interaction averages 90 seconds; physicians average 45/day |
| Patient time lost | 21% of appointment time is documentation-facing, not patient-facing |
| Error rate | Documentation-related adverse events account for 1 in 5 preventable hospital errors |
The root cause is misaligned architecture. Electronic Health Record systems were designed to satisfy billing requirements, not clinical workflows. The ICD-10 code exists to produce a reimbursement claim — not to describe what happened in the room. The physician has become the data entry point between clinical encounter and billing system, and no amount of voice recognition bolted onto a 30-year-old database architecture has fixed that.
MedConsult AI was built from a different premise: the encounter is the source of truth, and documentation should emerge from it — not be produced by the physician after it concludes.
Platform Architecture
┌──────────────────────────────────────────────────────────────────┐
│ MedConsult AI Platform │
│ │
│ ┌──────────────────────────────────────────────────────────────┐ │
│ │ Practitioner Dashboard │ │
│ │ Encounter Hub · Documentation Review · Patient Comms Hub │ │
│ └──────────────────────────────────────────────────────────────┘ │
│ │ │
│ ┌──────────────────────────────────────────────────────────────┐ │
│ │ AI Processing Layer │ │
│ │ Ambient Transcription → Clinical NLP → SOAP Generator │ │
│ │ Symptom Extraction → Differential Engine → Rx Draft │ │
│ └──────────────────────────────────────────────────────────────┘ │
│ │ │
│ ┌──────────────────────────────────────────────────────────────┐ │
│ │ Compliance & Security Layer │ │
│ │ PHI Isolation · HIPAA Encryption · Audit Trail · RBAC │ │
│ └──────────────────────────────────────────────────────────────┘ │
│ │ │
│ ┌──────────────────────────────────────────────────────────────┐ │
│ │ Integration Hub │ │
│ │ EHR APIs · Patient Portal · Billing Systems │ │
│ └──────────────────────────────────────────────────────────────┘ │
└──────────────────────────────────────────────────────────────────┘
The architecture enforces a single principle: AI does the documentation work; the physician does the clinical work. Every module was designed to minimize keystrokes, clicks, and context switches between clinical judgement and written record.
Four core modules:
-
Encounter Intelligence — Ambient AI that listens to the clinical encounter, structures the conversation in real-time, and generates a draft SOAP note before the patient leaves the room.
-
Documentation Review — The physician reviews AI-generated drafts with one-click approval, targeted edits, or full override. Nothing is finalized without physician sign-off. The AI speeds the process; the physician owns the output.
-
Patient Communication Hub — After-visit summaries, prescription instructions, follow-up scheduling, and referral communications — all drafted by AI, reviewed by the practitioner, dispatched via HIPAA-compliant channels.
-
Compliance & Audit Console — Every AI action, every edit, every approval is logged with physician identity, timestamp, and confidence score. The audit trail is immutable and exportable for HIPAA review.
AI Consultation Engine
The consultation engine is the core technical innovation. It does not record a transcript and summarize it — a solved problem available in any commodity AI API. It understands the clinical encounter as a structured event with medical semantics.
Ambient Transcription with Clinical Intent Detection
The transcription layer does more than convert speech to text. It identifies:
- Speaker roles: physician vs. patient vs. family member
- Clinical assertions: symptoms, duration, onset, severity, anatomical location
- Existing conditions: confirmed diagnoses referenced in conversation
- Medications mentioned: names, dosages, compliance indicators
- Examination observations: physician findings stated aloud during physical exam
- Patient concerns: expressed worries, preferences, and decision-relevant questions
This intent structure feeds a clinical NLP pipeline that maps entities to medical ontologies — SNOMED CT for clinical concepts, RxNorm for medications, ICD-10 for diagnosis coding — in real-time.
SOAP Note Generation
The output of the clinical NLP pipeline is a structured SOAP note:
S (Subjective): Chief complaint + patient-reported history
O (Objective): Physician observations + vital signs (if integrated)
A (Assessment): AI-suggested differential (flagged as suggested, not definitive)
P (Plan): Treatment plan, prescriptions, referrals, follow-up
The Assessment section is always framed as a clinical suggestion — the AI proposes, the physician decides. This framing is not just ethical; it is the only approach that will survive regulatory scrutiny and physician trust simultaneously.
Differential Suggestion Engine
The platform optionally surfaces a ranked differential diagnosis list, generated from structured symptom and history data. Each suggestion includes:
- Relative confidence level (High / Moderate / Consider — not raw percentages)
- Supporting clinical entities from the encounter
- Contraindicated differentials based on stated medications or documented conditions
- One-click "add to assessment" or "dismiss with reason"
This is AI as a second set of eyes, not AI as a replacement diagnostic. The distinction matters to regulators, to physicians, and to the product's legal standing.
Compliance & HIPAA Architecture
Healthcare AI that is not architected for compliance from day one cannot be retrofitted. PHI isolation, data residency, breach notification, and access audit are not features — they are constraints that shape every technical decision from the first line of code.
PHI Data Architecture
Each practitioner tenant operates in a fully isolated data environment:
- Storage isolation: Each tenant's PHI is stored in a separate encrypted partition. Cross-tenant data access is architecturally impossible — there is no query path, no shared table, no API surface that could expose one tenant's PHI to another's context.
- Encryption: AES-256 at rest, TLS 1.3 in transit. Keys are tenant-specific and rotated on a 90-day schedule.
- Data residency: US-based data centers only. No PHI traverses international boundaries. Verifiable on request.
HIPAA Technical Safeguards
| Safeguard | Implementation |
|---|---|
| Unique user identification | MFA-enforced login, session tokens per device |
| Automatic logoff | 15-minute idle timeout on all dashboard surfaces |
| Audit controls | Every PHI access logged: user, timestamp, action, record ID |
| Integrity controls | SOAP notes hash-verified; tampering is detectable and logged |
| Transmission security | End-to-end encryption on all patient communications |
Business Associate Agreement
MedConsult AI executes a HIPAA-compliant Business Associate Agreement with every healthcare customer. The BAA defines the technical commitments described in this section and makes them contractually enforceable — a prerequisite for any enterprise health system procurement.
AI Confidence Flagging
Every AI-generated clinical suggestion carries a confidence score and a mandatory physician review gate. The platform cannot finalize any clinical documentation without an authenticated physician sign-off action. This is not just compliance design — it is the mechanism that keeps AI in its appropriate role: assistant, not decision-maker.
Market Opportunity
Primary Market: US Physician Practices
There are approximately 1.1 million actively licensed physicians in the United States. Roughly 75% practice in settings where they bear direct responsibility for their own documentation workflow — solo practices, small-group practices, and employed positions without dedicated scribes.
At $299/month per provider, a 1% penetration of the addressable physician market represents $394M ARR. No single competitor currently offers an AI-native, HIPAA-compliant documentation platform at this price point with this feature set.
Adjacent Segments
| Segment | Licensed Practitioners | Opportunity |
|---|---|---|
| Nurse Practitioners & PAs | ~400K | Same documentation burden; same compliance requirements |
| Behavioral Health | ~178K licensed therapists | Session note generation; distinct clinical vocabulary |
| Physical Therapy | ~311K | Functional assessment documentation; outcome tracking |
| Urgent Care & Emergency | ~2,700 centers | High volume, high documentation burden; strong per-shift ROI |
| Telehealth Platforms | $79B market by 2030 | Embedded documentation layer; white-label licensing opportunity |
Enterprise Health System Upside
A 500-physician health system at $250/seat/month represents $1.5M ARR — a single deal. Enterprise contracts unlock EHR integration fees, implementation services, custom SLA agreements, and multi-year contract premiums. The practitioner-led demand signal is the most reliable path into enterprise procurement: administrators respond to internal champions, not cold outreach.
Go-to-Market Strategy
Phase 1: Practitioner-Led Growth
Individual physicians and small group practices offer the fastest purchasing cycle in healthcare. They sign up in minutes, see value in the first encounter, and become the most credible sales channel for their professional network.
Channels: medical community forums, CME content partnerships, physician-facing LinkedIn, clinical podcast sponsorships, peer referral incentives.
Phase 2: Group Practice Expansion
Solo practitioners who adopt create inbound demand from their practice administrators. The administrator conversation centers on billing compliance, HIPAA audit readiness, and ROI quantification: physician time recovered, scribe costs eliminated, malpractice documentation strengthened. This is where the compliance architecture becomes a sales asset — the platform's HIPAA documentation package is ready before the legal question is asked.
Phase 3: Enterprise Health System
Enterprise deals follow the same pattern at scale — extended evaluation cycles, procurement processes, integration requirements, and institutional legal review. MedConsult AI is positioned as the clinical intelligence layer: the AI infrastructure on which the health system's documentation workflow runs.
Pricing Architecture
| Tier | Price | Target |
|---|---|---|
| Solo | $299/month | Individual practitioners |
| Practice | $199/seat/month (5-seat minimum) | Small group practices |
| Enterprise | Custom (volume + integration + SLA) | Health systems, hospital networks |
The tiered model enables viral solo adoption at accessible price points while preserving significant enterprise pricing upside as the platform scales.
That’s the full picture.
More from The Studio
All Papers →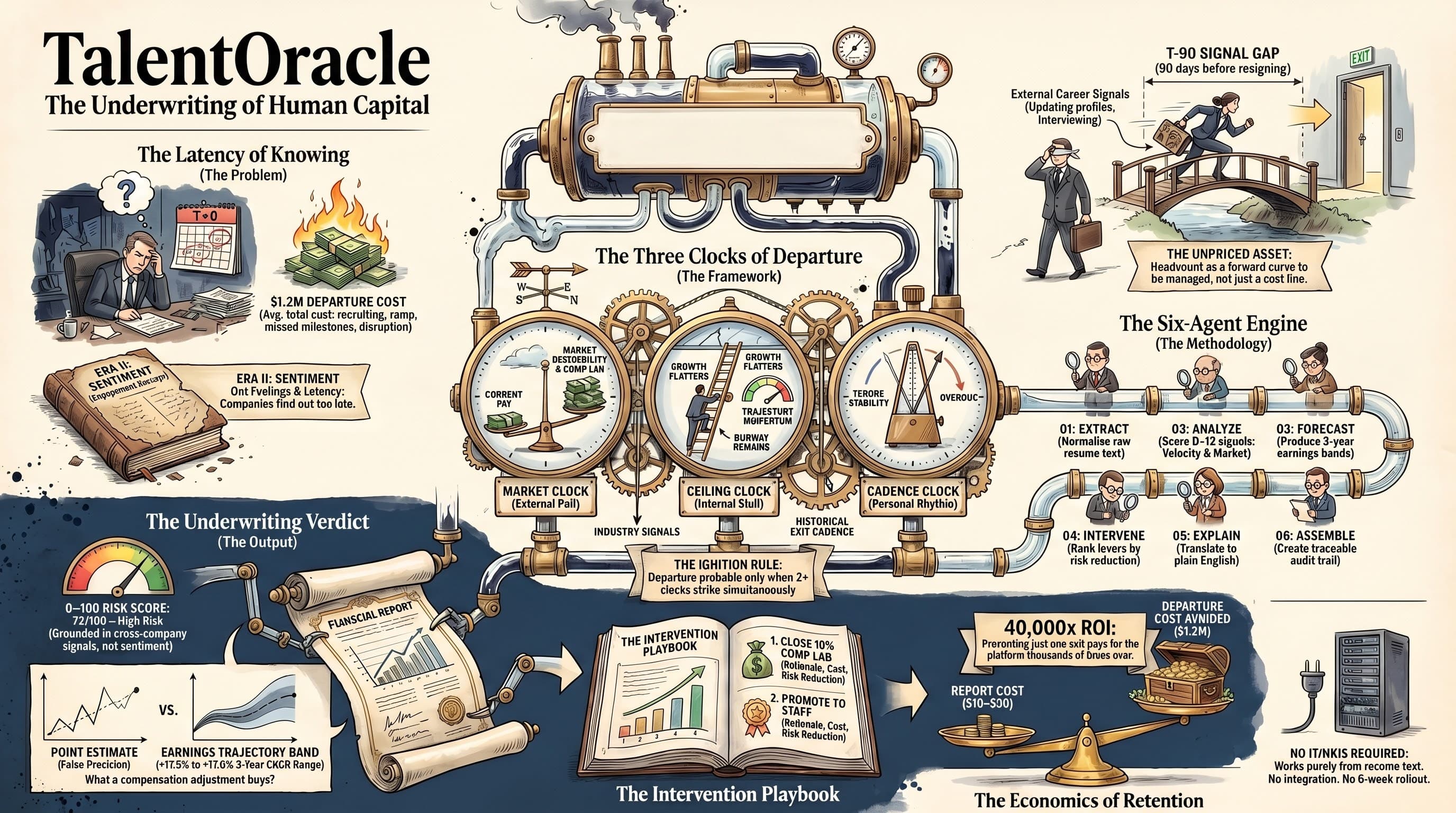
TalentOracle: The Underwriting of Human Capital
The average cost of a senior employee departure is $1.2M when recruiting, ramp, missed milestones, and team disruption are fully loaded. Most companies absorb this cost in silence because they found out too late. TalentOracle is a six-agent AI platform that predicts employee departure 90 days before it happens — using only resume text, with no HRIS integration, no survey, and no manager disclosure required. This paper sets out the Three Clocks of Departure framework, the six-agent engine architecture, the Underwriting Verdict output format, and the economics that make proactive retention the highest-ROI intervention a CHRO can make.

BISO: The Autonomous Security Immune System
BISO — the Bug Immune System — is an autonomous security platform that combines Semgrep, CodeQL, and Snyk scanning with AI-powered vulnerability prediction, autonomous blue-red-judge fix cycles, and semantic bug memory that learns from every outcome. This paper maps the immune system architecture, the self-healing fix loop, the topology-aware prediction model, and the structural case for autonomous AppSec as the successor to reactive vulnerability management.
Want to go deeper?
Discuss this paper with my digital twin.
Ask questions, challenge the framework, explore implications.
Open the Digital Twin